
How Can We Help?
Acute coronary ischaemia
Introduction
Coronary ischaemia is frequently missed because of either atypical presentations or because clinicians simply forget to consider it. Remember that pain my be atypical or absent altogether in diabetics, particularly diabetic women, and that epigastric pain should not be automatically labelled as due to peptic ulcer disease without giving serious thought to the possibility of myocardial ischaemia.
If in doubt, do an ECG. If still in doubt, do another one an hour or so later. Biomarkers of cardiac damage (e.g. troponins) were designed to be used to exclude ischaemic heart disease (i.e. in the emergency room setting, a normal troponin in the setting of equivocal other evidence for ischaemia would make the diagnosis unlikely); finding an elevated toponin result the next day in a patient with obvious ST changes is seldom helpful. Serial emergency department troponin measurements, even if rapidly available, do not seem to improve safety1. The value of repeat measurement is not clear in established ischaemia.
There are also other causes for elevated troponin levels, such as heart failure, where persistent elevation does have prognostic value2 Other causes of elevation include renal failure, pulmonary embolism, stroke and rhabdomyolysis)3

Acute coronary syndromes
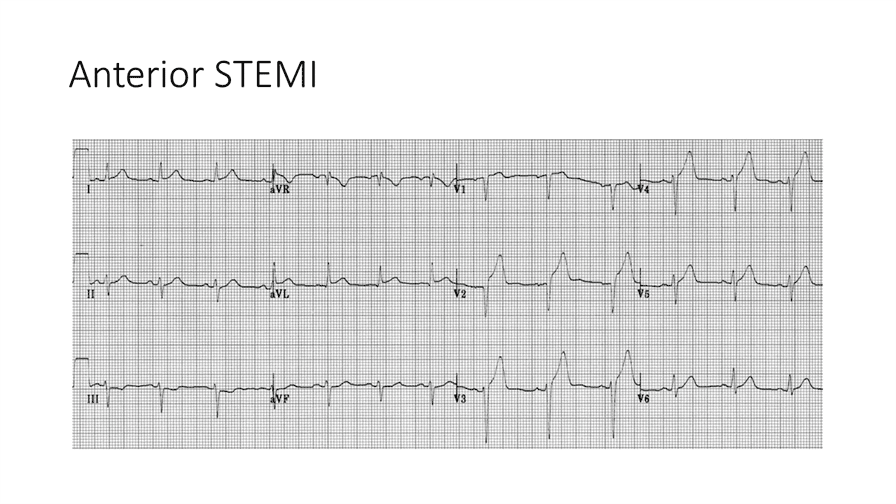
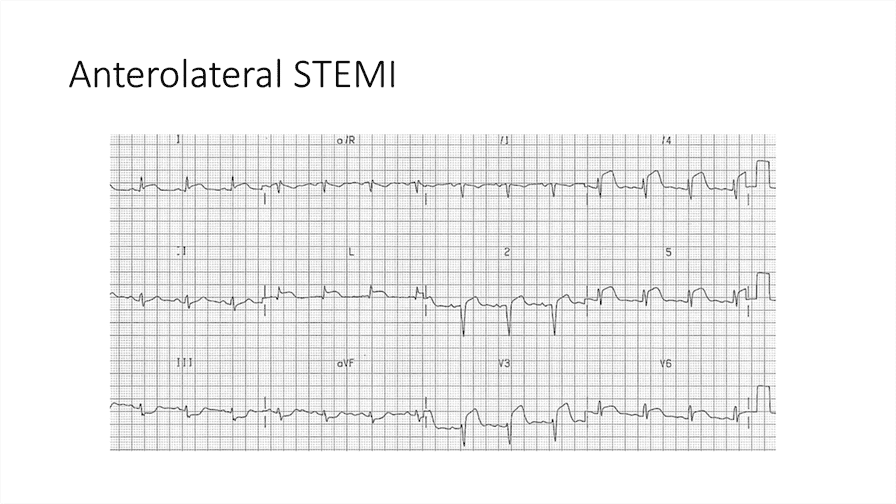
The acute coronary syndrome has three diagnostic components at presentation; these are re-allocated with time and the acquisition of further information about the patient. The key procedure which is often forgotten is the need to re-do the ECG after 4–6 hours, or earlier if you are concerned. Looking carefully at the ECG is very important – the key features to look out for are ST elevation, ST depression, and T wave flattening or inversion.
High risk :
History: – > 50; male; smoker; diabetic; dyslipaemia; previous MI or hypertension; family history IHD.
Exam: pulse > 100; low BP, poor peripheral circulation
(STEMI = ST elevation myocardial infarction; NSTEMI = non ST elevation myocardial infarction; UAP = unstable angina. The development of Q waves can occur in both STEMI and NSTEMI; their presence is indicative of more extensive myocardial damage – a so-called transmural MI.)
Unstable angina and NSTEMI
The acute coronary syndromes of unstable angina and NSTEMI are differentiated based on cardiac damage markers that are not always rapidly available; options in this situation are either to refer the patient to a place where they are, or to manage both possibilities as NSTEMI. Hospitals that do not allow the rapid determination of markers generally don’t have the same bed pressures as larger institutions, so err on the side of safety.
Management of NSTEMI
Aspirin 150 mg stat then 150 mg daily orally (ongoing) and clopidogrel 300 mg stat then 75 mg daily but the latter for just 3 months.
Simvastatin 40 mg daily
Enoxaparin 1 mg/kg every 12 hours – e.g. 80 mg SC 12 hourly if the patient weighs 80 kg. If using unfractionated heparin: give a bolus of 5000 units (strictly, 60 units/kg) then either an infusion of about 1000 units per hour, or as a subcut dose of 12 000 units 12 hourly, if an infusion pump is unavailable. Heparin does not reduce mortality, and only has a short-term effect on re-infarction rate (at 6 days.) if followed up for longer, this effect is no longer apparent.
Sublingual isosorbide 5 mg for pain as needed.
(There is an ABCDE mnemonic1 that may help one remember management components: A = aspirin + anticoagulation (heparin) + ACE inhibition (if EF<40%); B = beta-blocker + blood pressure control; C = cholesterol treatment + cease cigarettes + clopidogrel; D = diabetes management + diet (reduce weight to target BMI) and E = exercise.)
ST elevation myocardial infarction
Aspirin 150 mg stat and then 150 mg daily, also clopidogrell 75 mg daily but the latter only for one month.
Intravenous access
Supplemental oxygen is only necessary if there is evidence of hypoxaemia (basal crackles or sats <94%)
Morphine 10 mg diluted to 10 ml with 9 ml of saline; inject in 2 mg (2 ml) increments IVI until comfortable.
Simvastatin 40 mg daily
If less than 6 hours since the onset of pain, give streptokinase 1.5 million units in 100 ml normal saline over 30 minutes unless there are contra-indications. IF BP drops slow the infusion in the short term but try to give it within 60 minutes. (Note that because of antigenicity, streptokinase should not be given again if more than 5 days and less than 2 years since last infusion.) In patients not given streptokinase, consider heparin (dose as in NSTEMI) but benefit not particularly clear. (see the link below on perspectives in management for more details)
Nitrate therapy is usually prescribed sublingually as needed (Isosorbide 5mg SL); ongoing pain may respond to intravenous therapy but this medication does not affect mortality.
Consider starting an ACE inhibitor (e.g. enalapril) early (within 36 hours) – main benefit (0.5% mortality reduction in the first month2) was seen in those with systolic BP > 120, pulse >80 bpm. Keep on an ACE inhibitor long term if evidence of LV dysfunction clinically or on Echo; the long term benefit in patient with normal LV function and no other indication for an ACE inhibitor is less clear, particularly if all other medications for CVS risk reduction are already being given.
Atenolol 50 mg orally. Unless there are strong contraindications such as a known history of asthma, try to start all patients on a beta-blocker as soon as haemodynamically stable and certainly prior to discharge so that you can assess tolerability before the patient leaves the ward. Clearly, some common sense is needed in the situation of patients with bradyarrhythmias or inferior infarction. (Beta-blockers have not been shown to confer a survival advantage when given in the first 24 hours, and the 45 000 patient COMMIT trial showed a clear, very early increase in cardiogenic shock in patients given intravenous metoprolol on admission. It is however advisable to start treatment within the first few days, as there is evidence of reduced mortality in that context, mainly due to reduced re-infarction and ventricular fibrillation.)4
A small dose of furosemide to start with (e.g. 20 mg) is only needed if there is evidence of congested lungs. Don’t confuse a few hypostatic crackles with pulmonary oedema.
Click here for perspectives on the actual value of various medicines in coronary syndromes https://medeval.co.za/wp/ischaemic-heart-disease-treatment-perspectives/
Choosing when to start a statin in patients who have not yet had a cardiovascular event (primary prevention)
Primary prophylaxis is a value judgement incorporating patient opinion on risk and benefit, and entails making a call on an event threshold. The usual underlying calculation is based on 10 year risk of a MACE (Major Adverse Cardiovascular Event). This threshold can be set anywhere – 20%, 15%, or even (NICE 2023)5 10%. From a treatment perspective however, the key figure is not so much the absolute figure as the expected benefit from treatment
There are a number of calculators offering slightly different perspectives on this benefit; one that is easy to use and to do ‘what if’ analysis (what if we added a statin) is found here.
An individual with multiple risk factors (diabetes, smoking, hypertensive, overweight, for instance) who also has an elevated cholesterol will benefit from lowering the latter, but not nearly as much as the cumulative effect of addressing all risk factors. This is shown in the figure below. For two heavy smokers, one an obese diabetic male, and the other a normal weight woman, both 60 years old, the key intervention is to stop smoking – it nearly halves absolute risk for the male, and does so entirely for the woman. However their pre-intervention risks are dramatically different – 10 year CVS event rates of 25% versus 10%. The end result of that is that while addressing all our other conventional risk modifiers (cholesterol, weight, blood pressure) makes considerable sense with a 25% baseline risk, and if all of these changes are achieved, drop risk to about 12%, for the woman with a starting risk of 10%, stopping heavy smoking drops this to 5% and all the other potential interventions make at most an extra 1% absolute difference in 10 year risk. In some such patients, the drawbacks of intensive treatment may be seen as outweighing potential gain.

Atypical chest pain
Pulmonary embolism can cause pain similar to ischaemic heart disease, but it can also appear ‘musculoskeletal’, even with localised chest wall tenderness, or pleuritic. The key issue is to think of it – it belongs in the differential diagnosis of most acute chest discomfort presentations.
Musculoskeletal pain is sharp and worsened by particular movements, and associated with areas of localised tenderness. There may be a history of sudden heavy lifting or other strain, or of relatively minor trauma.
Pleuritic pain is sharp and clearly related to breathing, but you have to bother to ask. Patients will be very clear on this issue.
Fibromylagic pain is often dull, although occasionally described as knife-like. It is constant and has usually been present for considerable time. It is present at rest, and even sometimes on wakening. It responds poorly to analgesics.
Pericarditic pain is sharp and central and of recent onset. It may be worse on sitting forward. Patients have often been given antacids as the pain radiates to the epigastrium.
Zoster pain is radicular – it is unilateral and clearly radiates along the distribution of a single thoracic nerve root. There may initially be no vesicles, and even when they do appear, they can be relatively inconspicuous.
Pain from osteoporotic vertebral settling with nerve root compression is very severe and of abrupt onset. There may be localised vertebral tenderness, but the root symptoms are sometimes bilateral.
Oesophageal pain is clearly related to swallowing if due to obstruction or thrush. When associated with hiatus hernia and reflux, it tends to be dull, and may even radiate down the left arm. It is worst at night on lying down after a big meal, but needs to be distinguished from Prinzmetal’s angina, which also often comes on at night. Oesophageal pain is often relieved by nitrates.
Pain from aortic dissection is described as very severe, sharp or tearing, and may be associated with missing or reduced pulses and a background of hypertension. The plain CXR may be suggestive (abnormal contour of aortic arch) but ultrasound or CT is usually necessary to make the diagnosis.
-
Gluckman TJ, Sachdev M, Shulman SP, et al. A simplified approach to the management of non–ST–elevation acute coronary syndromes. JAMA. 2005;293:349–57. ↩︎
-
ACE Inhibitor Myocardial Infarction Collaborative Group. Indications for ACE inhibitors in the early treatment of acute myocardial Infarction. Systematic overview of individual data from 100 000 patients in randomized trials. Circulation. 1998;97:2202–2212. ↩︎
Wassie M, Lee M, Sun BC, et al. Single vs Serial Measurements of Cardiac Troponin Level in the Evaluation of Patients in the Emergency Department With Suspected Acute Myocardial Infarction. JAMA Netw Open. 2021;4(2):e2037930. doi:10.1001/jamanetworkopen.2020.37930 ↩
O’Connor CM, Fiuzat M, Lombardi C, et al. Impact of serial troponin release on outcomes in patients with acute heart failure: analysis from the PROTECT pilot study. Circ Heart Fail 2011;4:724–32 ↩
Mahjan VS, Jarolim P. How to interpret elevated cardiac troponin levels. https://doi.org/10.1161/CIRCULATIONAHA.111.023697 ↩
Chen ZM, Pan HC, Chen YP, Peto R, Collins R, Jiang LX, Xie JX, Liu LS; COMMIT (ClOpidogrel and Metoprolol in Myocardial Infarction Trial) collaborative group. Early intravenous then oral metoprolol in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet. 2005 Nov 5;366(9497):1622-32. doi: 10.1016/S0140-6736(05)67661-1. PMID: 16271643. ↩
O’Dowd A. NICE recommends wider use of statins to cut cardiovascular risk. BMJ. 2023 Jan 12;380:89. doi: 10.1136/bmj.p89. PMID: 36634930. ↩