
How Can We Help?
Diabetes mellitus

Diabetes is becoming more common, with most of the burden of disease being due to the rising epidemic of type 2 diabetes. Prevalence rates in urban and peri-urban areas are at least 6%, and about 25% of newly diagnosed type 2 diabetics may already have retinopathy, and 20% of type 1 diabetics may have nephropathy, which is a leading cause of death in this group.1 There are an estimated 2 million or more people in South Africa living with diabetes. (2017 JEMDSA Guideline)
Definitions
The American Diabetes Association allows diagnosis of diabetes based on HbA1c (>.6.5%), a fasting plasma glucose of more than 7 mmol/l or a glucose of more than 11.1 mmol/l two hours after a glucose load of 75 g, or a random glucose of the same level. :
- If the random blood sugar (lab or finger prick) is greater than 11 mmol/l, then the patient is diabetic.
- If the fasting sugar is > 7 mmol/l, then the patient is diabetic.
- If the random sugar is < 11 and the fasting sugar is < 7 (not that common an occurrence) then do a 75 g oral glucose tolerance test. If the 2 hour value is >11 the patient is diabetic, and if it is between 7 and 11, the patient has ‘IGT’ or impaired glucose tolerance (increased CVS risk).
The WHO HEARTS-D document (download here) provides definitions for a few more types of diabetes besides Type I, Type II and gestational. Of interest are the hybrid forms (ketosis prone Type II, and slowly evolving immune mediated diabetes of adults) and those associated with pancreatic damage either from viral infections (Covid-19 being a good example) or alcohol use (often associated with exocrine pancreatic insufficiency, and very sensitive to development of hypoglycaemia due to very poor energy reserves.)
Practical issues with measuring fingerprick glucose.
Machines are simpler and quicker now, so errors are less. However beware of deeply vasoconstricted (e.g. cyanosed digits, where getting back a hypoglycaemic reading is not uncommon – check with blood from the antecubital fossa.) 2
At the other extreme, alcohol swabs don’t necessarily clean hands of glucose – residual sugar from handling/peeling fruit is removed by washing with soap and water, but not entirely by alcohol swabs3
Aim of therapy
The aims of controlling diabetes are to reduce complication rates and allow patients, as far as is possible, to live normal life styles. In type II diabetes controlling energy intake and reducing low grade inflammatory responses probably have the most direct effect on the important cardiovascular and renal endpoints which are of concern, but the main issue with this illness is the very slow and indirect relationship between disease progression and onset of any symptoms which might cause concern amongst patient, making this nearly always a ‘catch up’ illness.
The clear hope was that agents having an impact on glucose levels would also lead to improvement in both macrovascular and microvascular endpoints; HBA1c has turned out to not be the successful surrogate it was hoped (certainly for macrovascular disease, where harm accumulates over years to decades.)4 However epidemiology studies continue to find a ‘sweetspot’ for both overall and cardiovascular mortality in Type II diabetes around an HbA1c of 7-7,9 %5 The field is currently influx, with high hopes being pinned on newer agents, and some former ‘ideal’ agents now being less favoured.
Diabetes mellitus – individualising therapeutic goals
The initial choice of agent in an overweight person should be metformin if renal and hepatic function is normal. Sulphonylureas may be added if control is inadequate, with the same caveats about renal and hepatic function. Most young people will need insulin rather than oral agents, and very thin patients, regardless of age, usually require insulin,.
Strict euglycaemia has been demonstrated to reduce the composite risk of complications in both Type 26 and Type 1 diabetes, regardless of the method used to lower the sugar.
In an environment ill equipped with telephones, community diabetic sisters, and home glucose monitoring, the mortality gains of strict control may be more than offset by complications of hypoglycaemia. (As an example of this perspective you would need to treat 31 patients for 10 years to prevent one diabetes related endpoint (NNT=31), but using sulphonylureas for this time period would cause 2 episodes of major hypoglycaemia. (NNH = 20) Control that is excellent for a motivated 25 year old may be singularly inappropriate for a 60 year old partially sighted person with poor social support and moderate renal impairment.7
Be wary of the patient with superb sugar control – consider renal failure or over treatment.
Hyperglycaemia is of most concern in the setting of an unstable patient – dehydration, infection or recent changes in medication.
Diabetes is primarily a disease of life-style, and attempts to get the obese person to eat less and lose weight seldom meet with success. Seeing patients like this monthly is arguably an inappropriate use of a scarce health care resource (you) and management at primary care level is usually appropriate. When they do return, however, treat them with extra care, as there is usually something else on the go.
Non-pharmacological therapy
Diet
Reducing intake is easily said and extremely difficult to do. One meta-analysis disconcertingly found that weight loss was linked to increased mortality in diabetics who were obese or overweight, unless this weight loss was intentional; this probably represents confounding by other conditions (e.g. malignancies) linked to weight loss.8
A more conventional result from a recent observational study in the UK linked a 13% reduction in weight in obese subjects with clear benefits in terms of dyslipidaemia, hypertension, sleep apnoea and diabetes.9
Exercise
Overweight patients with painful knees and hips struggle to follow exercise prescriptions, unless these are tailored to ability. Some exercise confers cardiovascular benefits beyond simply weight loss – perhaps via anti-inflammatory or other mechanisms.10
Pharmacological treatment
Starting medication should not be seen as a quick solution allowing less emphasis on lifestyle; on their own, the medications at the lower end of the cost spectrum are unlikely to have major cardiovascular risk reduction benefits.
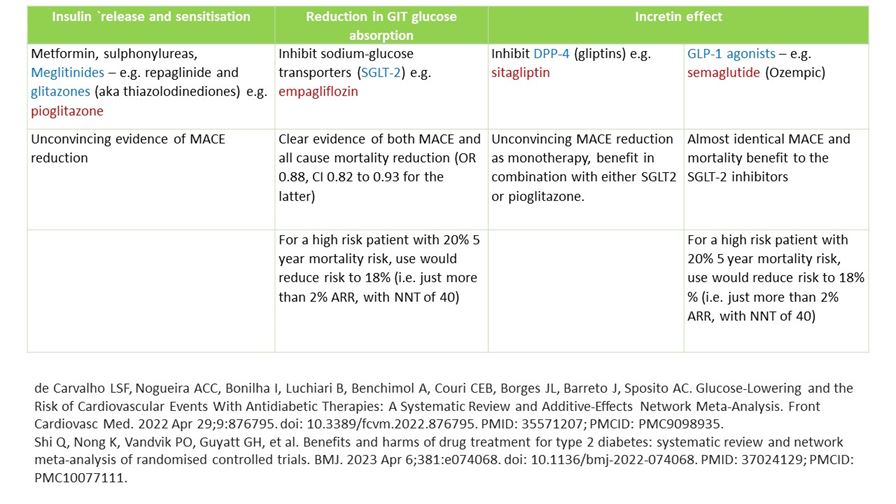
Newer agents in diabetes have taken similar directions to established products (e.g. the glitazones/thiazolodinediaones such a pioglitazone aim at insulin release and sensitisation, like metformin and the sulphonylureas, or have taken different approaches, such as reducing glucose absorption (SGLT2, sodium-glucose co-transporter inhibitors, or gliflozins) such as empagliflozin, or have an incretin effect. Incretins such as glucagon-like peptide (GLP-1) and glucose dependent insulinotropic polypeptide (GIP) respond to the presence of gastrointestinal glucose and promote serum glucose lowering and weight loss, with considerable publicity surrounding the GPL-1 agonist semaglutide (Ozempic). Inhibitors of incretin metabolism act on dipeptyl peptidases such as DPP-4 and are called gliptins (e.g. sitagliptin)
The key aim of therapy is to reduce disease complications and allow patients to live longer with better quality of life. A useful index of the efficacy of various agents is major adverse cardiac events (MACE) prevented, and in this space newer agents have better evidence:
Metformin
This agent is classically described as not associated with weight gain or hypoglycaemia. Weight loss is modest (about 3% of baseline is probably all that can be expected)11 However hypoglycaemia is described, although rare. Avoid if the GFR is less than 30 or if there is liver disease or alcohol abuse or uncontrolled heart failure.
Start with 500 mg twice daily to a maximum of 850 mg 8 hourly.
In patients on dolutegravir do not use more than a total of 1 g per day of metformin, as dolutegravir may increase serum levels of the agent.
Sulphonylureas
These are dangerous in patients with renal impairment as they may cause significant hypoglycaemia. Glibenclamide dosing is usually about 2.5 mg/d (30 mins before breakfast) increasing gradually to a max of about 10 mg per day, with more in the morning than the evening ( e.g. 5 mg mane, 2.5 mg before supper) Start glimepride at 1 mg daily and increase to about 4 mg per day if needed.
These agents almost certainly do not have a cardiovascular advantage, and perhaps even cause increased CVS risk, so they are becoming less popular as newer and likely more effective agents become available.12
Combining insulin and oral agents
This is commonly done, and goes in and out of fashion. In general it tends to complicate matters for rather unclear advantages. Better glucose control is relatively easy to achieve in most patients simply by increasing the insulin dose. A tenuous case can be made for adding a bit of metformin to Type II patients who are starting to gain weight excessively on insulin.
Incretins
Small polypeptides such as glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) known as incretins have been the target of research for more than a decade, and agonists such as semaglutide and tirzepatide not only have a role in diabetes per se but seems to have clear weight loss benefits as well. Whether these effects will translate into sustainable cardiovascular and mortality benefits are still not entirely clear13. The main issues remain acceptability (injections) and cost.
Efficacy of therapy
Although Type I and Type II diabetes share a common name, they are in many respects very different illnesses. However, therapy for both revolves around life-style adaptation. In IDDM the adaptation concerns learning to fit regular insulin use and dietary modification or awareness into a normal daily routine. In NIDDM, the issues are more complex and concern adjusting the other risk factors of obesity, smoking, hypertension and dyslipidaemia. Many of these goals can be met by exercise, better diet and weight loss, and in the absence of attention to these, drug endeavours are not dramatically effective.
Perspective – UKPDS (intensive glycaemic control with oral agents).
The UKPDS was a large, long-running trial looking at the use of oral agents to achieve good(ish) glucose control. It demonstrated that metformin use provided a survival advantage, and that in general tighter glucose control resulted in fewer diabetes-related events. UKPDS was unblinded, failed to demonstrate a mortality advantage from the use of sulphonylureas, and most of the accrued benefit was for microvascular and not macrovascular endpoints.14 The microvascular endpoints were part of a composite endpoint, which was difficult to interpret clinically, but consisted mainly of ‘episodes of photocoagulation prevented’ – the ARR for ‘any diabetes related endpoint’ was 3.2%, of which 2.7% were episodes of photocoagulation. All the other endpoints, including mortality and macrovascular complications, had to make do with a 0.5% ARR after 10 years of treatment.
Perspective – metformin and mortality – systematic review
Metformin is universally recommended as an agent of choice in obese patients with T2DM, based mainly on the mortality advantage UKPDS 34a, which compared metformin plus diet to diet alone. However UKPDS34b was similarly powered but compared metformin and a sulphonylurea with a sulphonylurea alone, and in this instance failed to demonstrate a total mortality benefit. A French group15 performed a systematic review of all metformin trials in T2DM and rather disconcertingly failed to demonstrate any benefit from metformin over a range of comparators (e.g. mortality risk ratio 0.99, 95% CI 0.75 to 1.31.) Admittedly there was significant heterogeneity, considerably variation in follow-up duration, and a disturbingly small total amount of trial evidence – 13 trials with 13 110 patients, 463 deaths. COSMIC, a one year post-marketing study in the US, contributed more than two thirds of the patients but less than a quarter of the outcomes.) As a take home message, the authors concluded that we still don’t really know if metformin saves lives but it may be better than the available alternatives.
Perspective – DCCT (intensive glycaemic control in insulin dependent diabetics)
This trial16 followed 1441 patients for a mean of 6.5 years on either twice daily insulin or intensive control with thrice daily insulin or an infusion pump. It should be noted that less than 5% of the trial cohort managed to keep their HbA1C below 6.05%, and only 44% reached that goal even once. The other aim was to have a fasting glucose of less than 6.7 and a post-prandial glucose of less than 10mmol/l. The result was no significant difference in mortality but a reduction in retinopathy, albuminuria, and neuropathy (NNT 6, 25, and 15 respectively.)
It is important to note that the outcomes chosen reflect disease progression and are clearly important, although they are all (except mortality!) surrogate endpoints – the degree of patient-perceived disability is not readily available. A subsequent article17 has attempted to give this perspective. Published in 1996, it suggested that the cost per QALY of intensive control would be $28 661. Although this fits in with US ‘affordable’ QALY expenditures, in most resource-constrained countries this would be regarded as quite costly.
Perspective – more intensive treatment and diabetic nephropathy
The practical difficulties of achieving recommended targets are nicely portrayed in a study from Scotland18 In this randomised controlled study patients with diabetic nephropathy either got ‘intensive’ treatment (N=47) where patients were seen as often as was needed in order to meet the treatment objectives, or were followed in a normal way (N=43). Treatment goals were the same in both groups (SBP <140, DBP <80, HbA1C <8%, (this is modest relative to DCCT) sodium intake <120 mmol/d, protein < 1g/kg/d and cholesterol <4 mmol/l).
Even with monthly visits as part of a controlled trial, run by presumably enthusiastic clinicians, 60% of patients failed to achieve target systolic BP. The extra work (19 versus 8 clinic visits per patient) resulted in lower systolic blood pressure (21 mmHg), better cholesterol control (68% reached target versus 46%), less smoking (12% versus 4%) but no difference in glucose control. The end result was fewer hospital admissions (43 versus 69) and slower rate of progression of kidney disease (0.14 versus 0.53 ml/min/month .) Contextualising this, glucose was not disastrously out of control even at the start of the trial, so the scope for improvement was modest.
The same theme was also evident in the preliminary results of 4-T19, which randomised patients on oral agents to the addition of either biphasic, prandial, or basal insulin, where the proportions of patients with HbA1C ≤. 6.5 at one year were 17%, 23% and 8% respectively.
Perspective – ACCORD and ADVANCE
Further information on tighter glucose control has emerged since UKPDS. Firstly, it should be emphasized that this was very tight control, and what follows does not indicate that conventional attempts at relatively vigorous control of blood sugar are misplaced. As a reminder, mean plasma glucose can be approximated from HbA1C by doubling the HbA1C and subtracting four. (MPG = 1.98 x HbA1c – 4.29)20
In the 11140 patient ADVANCE21 study of tighter control in Type II diabetes, there was a median follow-up of 5 years, and the intervention group had a mean HbA1C of 6.5 versus 7.3 in the controls. Mean age was 66 years. There was no difference in mortality, rates of macrovascular events, or retinopathy. However there was a significant 1.1% ARR in the nephropathy composite endpoint, which resulted in reduction in rates of microvascular complications at a cost of increased severe hypoglycaemia (2.7% versus 1.5%, ARR 1.2%.)
The more concerning ACCORD22 study included 10251 patients with a mean age of 62.2 years and slightly higher cardiovascular risk profiles. The achieved HbA1c of 6.4% was almost identical to that in ADVANCE. The trial was stopped early because of increased mortality (HR 1.22, 95% CI 1.01 to 1.46.) This translated into an absolute excess mortality of 1.1% per year. Rosiglitazone was used in 91% of the patients in the intensive treatment arm, and it has been suggested that this may have contributed to the mortality excess. Hypoglycaemia requiring assistance was also more common (10.5% versus 3.5%, p<0.001.)
Starting insulin in outpatients.
Working out the dose of insulin is associated with cabalistic formulae and abstruse calculations, some of which have been weakly validated in real life situations. However attempting to dose from formulae is a recipe for confusion. Formulae perform best as a way of setting a target dose to be aimed for after working up from smaller and safer doses. The advice given here applies to the stable patient being seen in a clinic, and not to an unstable patient requiring admission.
Diabetes secondary to chronic alcoholic pancreatitis is associated with relative lack of counter-regulatory hormones, and such individuals are prone to profound hypoglycaemia and should be admitted to start insulin. Most others can be started as outpatients, with a bit of care.
Decide on whether to use a basal-bolus regimen or a twice a day insulin mix regimen. The former consists of a twice a day basal injection of an intermediate acting insulin and a meal-related injection of a short acting agent. The latter involves giving a twice daily injection of a 30:70 mixture of short and intermediate acting insulins. A third option in the frail elderly where control without insulin proves impossible, is to give a single late night injection of an intermediate acting agent which will work the following day.
Either teach it yourself or make sure the patient gets adequate instruction from nursing colleagues on how to draw up and inject insulin.
Start the patient on low doses such as a total daily dose of 25% of body mass – e.g. 10 units mane and 5 units nocte for somebody weighing 60 kg and 6 units mane and 4 units nocte for somebody weighing 40 kg. Review in a few days to see how things are going. At repeat visits you should be focussing more on injection technique, meals and coping strategies for possible hypoglycaemia – the actual glucose level is not very important in that early stage.
Once the patient is safely established on a diet and injection routine, you can slowly increase the dose by 2-4 units per injection.
Sliding scales
It is far easier to control the blood sugar in a stable patient with twice or thrice daily meal-related insulin than with a sliding scale. Achieving perfect sugar control on a sliding scale is physiologically improbable.
Checklist:
- Is it really necessary? (If the patient is conscious and able to eat and drink, it probably ISN’T necessary. If the patient is really out of control (e.g. metabolic chaos due to infection or trauma), wouldn’t an insulin infusion be more appropriate?)
- Is it still necessary? (The need for a sliding scale should be reviewed daily)
- Is it working? (Reasons for failure are that it is not being followed, the doses or dose intervals are wrong, there is uncontrolled sepsis, or the caloric intake is too high)
- What are my criteria for stopping it? Aim to stop it when metabolic requirements become predictable, not when the sugar is well controlled.
- Write legibly in a place where the nursing staff can see it.
- Use lower doses for NIDDM patients and very low doses in chronic pancreatitis (no counterbalancing hormones like glucagon in the latter). Be cautious in chronic renal failure. As a rule, a sliding scale that is a bit too conservative can be fixed the next day, but one that is too aggressive may lead to irreversible neurological sequeli from hypoglycaemia.
- True insulin dependent diabetics should be able to get as much insulin with dosing at normal blood sugars, as their pre-morbid dose. For example, someone who is normally taking 80 units per day will inevitably go ketoacidotic if the suggested 4 hourly dose of insulin for a blood sugar of 10 mM is only 5 units (5 x 6 = 30 units/day, which is less than the patient’s non-stressed requirements!) It is perfectly possible to become profoundly ketoacidotic even if the blood sugar is not very high.
- Sliding scales are not writ in stone – they can be adjusted on a daily basis if you are not achieving what you want.
- A sliding scale that is needed for more than a few days is a cause for concern – something is being missed.
- Don’t forget that adequate fluid intake is very important – anyone on a sliding scale should have carefully thought out daily fluid prescriptions written, and previous day’s intake and output should be scrupulously reviewed.
The prescription should contain all of the following:
- Insulin type – e.g. short acting (e.g. Actrapid® or Humulin R®).
- Route – subcutaneous.
- Dose interval & blood (not urine!) sugar check interval should be stated.
- Choose a range of blood sugars that don’t overlap (i.e. not 10-15 and 15-20: what is the correct dose if the blood sugar is 15? Rather write 10-14.9 and 15-19.9.)
- State units of measurement for blood sugar in mmol/l.
- The heading of the insulin dose column should state the units – do not write ‘u’ after a number, as this can be interpreted as a ‘0’, and a dose 10 time what you intended is then given (‘4U’ becomes 40 units).
- All sliding scales should also include an evening dose of intermediate acting insulin of about 1/10th of body weight for Type I diabetics, and a morning dose of twice this. e.g. if 60 kg, give 6 units at night and 12 units in the morning. For Type II halve both doses – 3 units nocte and 6 units mane.
- Sign and date it.
Examples:
This is a guide only, and each scale should be tailored using the information above – there is no ‘right’ scale that works for all patients. (See the inside cover for an example of an insulin prescription and glucose monitoring chart that includes a basal dosing option.) In practice, outside a high care unit, 4 hourly SC sliding scales using only short acting insulin are not very effective at controlling glucose, as late night doses are often omitted and one is always playing ‘catch-up’ on a non-constant caloric intake. Sliding scales without some form of basal dosing are neither more effective (fixing hyperglycaemia) or safer23 (avoiding severe hypoglycaemia.)
If you have to:
Four hourly subcutaneous insulin sliding scale for a 50 kg Type I diabetic:
Daily intermediate acting insulin: 10 units mane and 5 units nocte. | |
Then 4 hourly sliding scale with short acting insulin as follows: | |
Finger prick blood sugar (mmol/l) | Units of subcutaneous short acting insulin |
0 – 3.4 | Give 50 ml of 50% DW if patient symptomatic and call the doctor. |
3.5 – 4.9 | Nil |
5 – 9.9 | 2 |
10 – 14.9 | 4 |
15 – 19.9 | 6 |
20 – 24.9 | 8 |
25 or more | 10 |
If more than 2 consecutive readings are > 25, call the doctor. |

Autonomic neuropathy in diabetes (DAN)
The main symptoms of autonomic neuropathy are: postural hypotension, gastric symptoms, diarrhoea, excessive sweating, bladder dysfunction and urinary retention, impotence, and cardiorespiratory arrests.24,25
Method of testing for autonomic neuropathy:
You need a sphygmomanometer and a cardiac monitor that displays instantaneous heart rate and allow you to print out a strip. (Do not try to use automated BP machines for this series of tests.)While the patient is lying down with the ECG connected, record a strip for a few respiratory cycles. Next measure the systolic BP. Get the patient to stand up and set the ECG going again to record about 40 beats. Stop the ECG, and ask the patient to remain standing until two minutes have elapsed. Record the systolic BP. Let the patient sit down, and do the heart rate response to Valsalva and the BP response to isometeric exercise. The entire process, including the calculations, should take about 10 minutes.
Max-min heart rate variation during deep breathing. The patient breathes in and out quietly (5 seconds in and five seconds out) while the ECG strip is running. Mark inspiration and expiration. Count the number of small blocks between two R wave peaks during expiration and divide this number by the number of small blocks between R waves in inspiration. A ratio > 1.17 is abnormal.
Heart rate response to standing. Normally heart rate speeds up to a maximum at 15 beats after standing and then slows most at the 30th beat. Count the number of small blocks between the peaks of the R waves for beats 30 and 31, and divide this by the number of small blocks between R waves 15 and 16.A ratio less than 1.03 is abnormal.
Postural drop. Measure the systolic BP lying down and then after standing for two minutes. An abnormal response is a difference between lying and standing systolic BP of more than 30 mmHg.
Diastolic BP increase with sustained handgrip. (Normally the BP rises because of increased cardiac output and unchanged peripheral resistance) Roll up a BP cuff, pump a little air into it, and ask the patient to squeeze it as hard as possible. Record the pressure reached. Then ask the patient to keep squeezing at one third of maximum for as long as possible (up to 5 minutes) Measure diastolic BP in the other arm before exercise, and then at 1 minute intervals during sustained handgrip. Subtract the pre-exercise reading from the highest reading during exercise. A difference of less than 15 mmHg is abnormal.
Heart rate response to Valsalva. Remove the plunger from a 10 ml syringe and attach the nozzle of the barrel to the rubber tubing of an aneroid (not mercury!) sphygmomanometer. Ask the patient to blow into the wide bore of the barrel hard enough to keep the pressure at 40 mmHg for 15 seconds, and record the ECG during and after. Count the number of small blocks in the longest RR interval and divide this by the number of blocks in the shortest RR interval. A value less than 1.2 is abnormal.
Symptomatic postural hypotension. Re-asses the need for diuretics or other anti-hypertensives which the patient may be taking. Elastic stockings plus fludrocortisone 0.1 mg/day. Advice to increase salt intake may also help. Both of these remedies only seem to work once peripheral oedema starts to appear, so beware of tipping the patient into cardiac failure.
gastric symptoms. More frequent smaller meals with reduced fat content. Metoclopramide 10 mg 3x/d is worth trying.
diarrhoea. A trial of metronidazole for three weeks may assist with intestinal overgrowth, but thereafter consider loperamide 2 mg 2-3x/d (although beware of causing toxic megacolon.)
bladder dysfunction and urinary retention. Frequent voiding. Supra-pubic pressure. Treat urinary tract infections. Prazosin or doxazosin may be worth trying.
impotence. Penile pressure/vacuum devices are available.
cardiorespiratory arrests. Beware, particularly related to anaesthesia.
Perspective – test performance in autonomic neuropathy
Good quality trials reporting sensitivity and specificity of the individual components of the test armamentarium are difficult to find. Common difficulties are selecting a group ‘thought to have autonomic neuropathy’ and comparing them with individuals thought to be normal (i.e. knowing the results before doing the test) and also the lack of a clear gold standard This may yield impressive numbers26. A more realistic set of figures from a group of uraemic (not diabetic) patients yielded sensitivities of 50% for heart rate response to Valsalva, 77% for heart rate response to breathing, 70% for heart rate response to standing, 15% for BP response to standing, and 77% for BP response to isometric grip.27 Reported specificities from other studies range from 60 to 100%, but again must be seen in the light of trial quality.
Diabetic ketoacidosis
Admission investigations:
U&E, glucose, serum ketones (beta-hydroxybutyrate), and venous blood gases if available.
Urine MC&S, blood culture.
Look hard for sepsis (UTI, infections on feet/ perineum, PID, ENT infections).
Fluids:
Normal saline (0.9%): 1 litre/hr in first and second hours, then 1 litre 2 hourly x 2, then 1 litre 4 hourly. At some stage, depending on clinical response, decrease to 6 hourly and then 8 hourly. Once the circulation is restored, there is little evidence that the infusion rate is particularly critical, but clearly be careful of continuing to pour fluids into individuals with cardiac failure or chronic renal failure – you will just add to the problems by precipitating pulmonary oedema.
Review fluids after 24 hours, or earlier if urine output less than 50 ml/hour, or there are signs of pulmonary oedema.
When blood glucose drops below 15 mmol/l, change to 5% dextrose saline at the same infusion rate as for N/S above, unless corrected sodium concentration is rising, in which case use 5% dextrose without the saline.
Potassium.
If urine output is more than 50 ml/hr, start replacing potassium from the third bag (i.e. once infusion rate has dropped to 1 litre 2-hourly) Mix 20 mmol of KCl in each litre from then on.
Heparin
In patients who are obese, dehydrated, and bedridden, heparin prophylaxis for the prevention of DVT seems a worthwhile, if unproven, strategy in this particular context. A dose of unfractionated heparin 5000 sc. units 8 hourly is adequate.
Sodium bicarbonate.
There is no convincing evidence that it is of clinical benefit and many theoretical reasons why it may be harmful – primarily worsening of intracellular and intracranial acidosis at the expense of correcting a serum surrogate. Avoid it.
Monitoring
Fingerpick glucose testing hourly, venous blood pH (Astrup) 4-6 hourly
Repeat U&E four-six hours after admission.
Insulin infusion:
Mix 100 u (one hundred units) of short-acting insulin in 1 litre of normal saline. (Or 20 units in 200 ml) Use an infusion controller (e.g. IVAC) and commence infusion at rate of 1 ml/minute = 6 units short acting insulin per hour. (Drop rate with 15 drop/ml giving set thus 15 drops/minute.) Alternatively, if a syringe driver is available, use it.
If hourly blood glucose trend is downwards, continue at this rate. If 2 glucose levels at hourly intervals are constant or rising, and glucose is still above 25 mmol/l, increase infusion rate to 8 units/hour (= 1.3 ml/minute = 20 drops per minute) then 10 or (rarely) 12. Ditto if pH not rising.
In situations where an infusion pump or other rate controlling device is unavailable, a reasonable alternative is to draw 50 units of regular insulin into a 20 ml syringe then draw up saline to a total volume of 20 ml. Then inject 5 units (2 ml) of this solution intramuscularly every hour (0.1 units/kg/hr). The reason for this work around is that you need a long needle for IM injections, but can only achieve subcutaneous positioning with a normal insulin syringe and needle.
Sliding scale:
Once the patient is awake and eating, and the pH is above 7.3, stop the insulin infusion and use a basal-bolus regimen as described under ‘sliding scales’. There is now also a case for starting intermediate insulin on admission.
Perspectives – DKA
Urinary ketones.
This test is often applied back to front – it is best at ruling out rather than ruling in the presence of DKA. In one study28 ketones were present in 99%, and had a specificity of 69% (LR+ 3.19, LR- 0.01) for the presence of DKA – i.e. their absence is a good excluder.
However the presence of urinary ketones is only a relatively weak indicator of the true presence of DKA (PPV 0.35) – you need another biochemical test such as a venous blood gas analysis or serum ketones to rule in the diagnosis. Many starved patients (even doctors post call!) may have ketonuria – this doesn’t mean that they necessarily have DKA.
Serum ketones
Serum ‘ketones’ comprise three different molecules; fingerprick test kits measure beta-hydroxybutyrate levels, which are normally less than 1 mmol/l. In DKA, levels are often between 4 and 12 mmol/l, but should fall by about 1 mmol/l/hour if therapy is efficacious.29 Failure to drop by this amount suggests a need to increase the insulin infusion rate. In the absence of facilities to measure beta-hydroxybutyrate, a simple option is to test for acetoacetate and acetone using the normal urine ketostix and serum from a centrifuged blood sample.
Markers of ketosis.
Serum ketones. 3-hydroxy butyrate is probably the ‘best’ measure of ketosis, but acetone and acetoacetate are more readily measured. The presence of the latter confirms ketosis; their absence does not exclude the presence of the less easily measured 3-hydroxybutyrate.
Venous versus arterial blood gas analysis.
Over the years many unfortunate patients with DKA have been subjected to multiple arterial punctures to determine pH response to therapy. Intuitively, this was always somewhat odd, since it is the response rather than the absolute value that is important in guiding therapy. A recent study30 (admittedly only looking at patients with initial pHs in the range 7.05-7.35) demonstrated good agreement between arterial and venous values, with the mean venous pH being 0.03 pH units lower than the arterial value. Mean venous bicarbonate was about 2 mmol/l higher than arterial. Unless there is an independent reason to look at serial arterial oxygen concentrations, it is unnecessary to do serial arterial gases in DKA.
Bicarbonate.
The literature consensus on this can best be described as ‘no consensus’. There are multiple textbook references and review articles talking about the use of bicarbonate being ‘controversial’, but copping out and supporting its use in patients with pH less than 7.1. One review points out that is precisely in this subset of patients that bicarbonate may do most harm.31 Many of the studies are observational, and because of possible selection bias, are particularly unsuited to answering this type of question.
Trial | Bicarb | Control | Primary outcome | Comment |
Lutterman | 12 | 12 | Difference in mean pH at various times | Unusual randomisation method, varying insulin doses |
Hale | 16 | 16 | Mean pH rise in 2 hrs | Study follow-up only lasted 2 hours |
Morris | 10 | 11 | Time to pH>7.3 | Unblinded. Controls sicker |
Gamba | 9 | 11 | Rate of rise of pH | Blinded, placebo controlled but too small. Surrogate endpoints |
A systematic review36 noted this lack of evidence of benefit, and raised concerns that it may actually do harm, particularly in children. Its continued use says more about the therapeutic desires of prescribers than the benefits of the medication.
Normal saline or hypotonic fluids?
The literature on this consists almost entirely of personal recommendations and reviews, often based on very plausible sounding theoretical considerations. Good quality trials comparing pertinent clinical outcomes in adults using different infusion regimens (rates and types of fluids) are scanty. There is an initial normal then half normal saline school, a Ringer’s school, and an entirely normal saline school, all with cogent arguments and weak or non-existent data (other than in laboratory animals). The paediatric literature is no better.
In the absence of empiric information, it would seem reasonable to replace with saline initially, and then be guided by corrected sodium response: a rising corrected sodium would be an indication for infusing fluids of reduced tonicity, whereas a stable or falling sodium in a clinically improving patient would lead to less need to swap away from saline. Once the glucose is down it is usual in any event to swap to dextrose saline.
One aspect of the dispute is that during episodes of dehydration the brain generates idiogenic osmoles to preserve its own water content (it sucks harder!) If markedly hypotonic fluid is then infused, reactive cerebral oedema may be a clinical problem.
Mortality in DKA.
Some US series are claiming figures of less than 5%; more traditional series have quoted up to 20% or even higher. The differences are largely related to referral patterns – young mildly ketotic individuals presenting early with a mean pH of 7.3 will clearly do better than the situation more commonly seen in resource-constrained countries where one fairly commonly encounters late presenting markedly dehydrated septic individuals with pHs of 6.9 or less, glucose concentrations up to 60 mmol/l and corrected sodium concentrations of 180 mmol/l.
Hyperosmolar non-ketotic states
The medical management of this is broadly similar to that of DKA, except that the emphasis should be more on volume replacement and somewhat less on insulin. Due to the presence of relative insulin resistance, sepsis, and poor intake, it is quite common to encounter some degree of ketosis. The key is that once sepsis is under control, the glucose drops very rapidly, and insulin requirements over the next few days may be quite modest.
Fluid replacement in patients with background cardiorespiratory disease.
The enthusiasm for very rapid saline infusion needs to be dampened somewhat when too rapid replacement may cause pulmonary oedema. Once blood pressure has been restored, more gentle fluid replacement is often adequate (e.g. 3 litres per day) and there are theoretical advantages, in terms of excess salt load, for using dextrose saline or dextrose once initial resuscitation is successful. Don’t forget the simple option of oral or nasogastric administration of tap water. A bit of care and regular (scheduled!) auscultation of lung bases usually leads to quite smooth recovery.
Peripheral vascular disease and foot care
Other than a few zealots, most doctors in busy environments are rather bad at focusing on foot care in diabetics. Getting one or more members of nursing staff enthusiastic about this aspect of care is very rewarding, but a few basics may help:
Diabetics with poor mobility and poor vision may not be quite sure what is going on with their feet – getting another member of the household involved may help.
- Examine diabetic patients routinely for evidence of peripheral sensory loss.
- When diabetics complain about their feet, take a look. Relatively innocuous little wounds can cause problems quite quickly. The lifetime prevalence of foot ulcers in this group has been estimated at 25%.37
- Minor trauma happens to feet quite often over decades, so diabetics experiencing their first episode of foot sepsis or ischaemia are often quite surprised – little injuries of this nature usually healed fine in the past.
- Careful pedicure helps, as does stopping smoking.
- Minor sepsis should be taken seriously and treated adequately with regular dressing and regular review. It doesn’t go away if ignored.
- Sepsis combined with poor circulation and poor glucose control is a particularly fertile ground – outpatient management is often inadequate so don’t be shy to admit such individuals – you may prevent an am
Beran D, Yudkin JS. Diabetes care in sub-Saharna Africa. Lancet. 2006;368:1689-95 ↩
El Khoury M, Yousuf F, Martin V, Cohen RM. Pseudohypoglycemia: a cause for unreliable finger-stick glucose measurements. Endocr Pract. 2008 Apr;14(3):337-9. doi: 10.4158/EP.14.3.337. PMID: 18463040. ↩
Takahisa Hirose, Tomoya Mita, Yoshio Fujitani, Ryuzo Kawamori, Hirotaka Watada; Glucose Monitoring After Fruit Peeling: Pseudohyperglycemia When Neglecting Hand Washing Before Fingertip Blood Sampling: Wash your hands with tap water before you check blood glucose level. Diabetes Care 1 March 2011; 34 (3): 596–597. https://doi.org/10.2337/dc10-1705 ↩
Hasan F, Hasan B. Antidiabetic medications and mortality reduction: a shift from surrogate to clinical endpoints. Ther Adv Endocrinol Metab. 2017 Dec;8(12):173-174. doi: 10.1177/2042018817737955. Epub 2017 Nov 7. PMID: 29238516; PMCID: PMC5721968. ↩
Raghavan S, Vassy JL, Ho Y, et al. Diabetes Mellitus–Related All‐Cause and Cardiovascular Mortality in a National Cohort of Adults. https://doi.org/10.1161/JAHA.118.011295Journal of the American Heart Association. 2019;8:e011295 ↩
UK Prospective Diabetes Study Group. Intensive blood glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes. Lancet. 1998;352:837-53 ↩
McCormack J Greenhalgh T. Seeing what you want to see in randomised controlled trials: versions and perversions of UKPDS data. BMJ. 2000;320:1720-3 ↩
Chen Y, Yang X, Wang J, Li Y, Ying D, Yuan H. Weight loss increases all-cause mortality in overweight or obese patients with diabetes: A meta-analysis. Medicine (Baltimore). 2018 Aug;97(35):e12075. doi: 10.1097/MD.0000000000012075. PMID: 30170423; PMCID: PMC6392938. ↩
Haase, C.L., Lopes, S., Olsen, A.H. et al. Weight loss and risk reduction of obesity-related outcomes in 0.5 million people: evidence from a UK primary care database. Int J Obes 45, 1249–1258 (2021). https://doi.org/10.1038/s41366-021-00788-4 ↩
Gleeson, M., Bishop, N., Stensel, D. et al. The anti-inflammatory effects of exercise: mechanisms and implications for the prevention and treatment of disease. Nat Rev Immunol 11, 607–615 (2011). https://doi.org/10.1038/nri3041 ↩
Elisa Lazzaroni, Moufida Ben Nasr, Cristian Loretelli, Ida Pastore, Laura Plebani, Maria Elena Lunati, Luciana Vallone, Andrea Mario Bolla, Antonio Rossi, Laura Montefusco, Elio Ippolito, Cesare Berra, Francesca D’Addio, Gian Vincenzo Zuccotti, Paolo Fiorina, Anti-diabetic drugs and weight loss in patients with type 2 diabetes.Pharmacological Research. 171,2021, 105782,ISSN 1043-6618, https://doi.org/10.1016/j.phrs.2021.105782. ↩
Scot H Simpson, Jayson Lee, Sabina Choi, Ben Vandermeer, Ahmed S Abdelmoneim, Travis R Featherstone. ,Mortality risk among sulfonylureas: a systematic review and network meta-analysis. The Lancet Diabetes & Endocrinology,2015,3; 43-51,ISSN 2213-8587,https://doi.org/10.1016/S2213-8587(14)70213-X ↩
John R. Ussher, Amanda A. Greenwell, My-Anh Nguyen, Erin E. Mulvihill; Cardiovascular Effects of Incretin-Based Therapies: Integrating Mechanisms With Cardiovascular Outcome Trials. Diabetes 1 February 2022; 71 (2): 173–183. https://doi.org/10.2337/dbi20-0049 ↩
McCormack J Greenhalgh T. Seeing what you want to see in randomised controlled trials: versions and perversions of UKPDS data. BMJ. 2000;320:1720-3 ↩
Boussageon R, Supper I, Bejan-Angoulvant T, Kellou N, Cucherat M, et al. (2012) Reappraisal of Metformin Efficacy in the Treatment of Type 2 Diabetes: A Meta-Analysis of Randomised Controlled Trials. PLoS Med 9(4): e1001204. doi:10.1371/journal.pmed.1001204 ↩
The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977-86 ↩
DCCT Research Group. Lifetime benefits and costs of intensive therapy as practiced in the diabetes control and complications trial. The Diabetes Control and Complications Research Group. JAMA. 1996;276:1409-15 ↩
Joss N, Ferguson C, Brown C, et al. Intensified treatment of patients with type 2 diabetes mellitus and overt nephropathy. Q J Med. 2004;97:219-27 ↩
Holman Rh, Thorne KI, Farmer AJ, et al. Addition of biphasic, prandial, or basal insulin to oral therapy in type 2 diabetes. N Engl J Med. 2007;357:1716-30 ↩
Rohlfing CL, Wiedmeyer HM, Little, RR, et al. Defining the relationship between plasma glucose and HbA1C. Diabetes Care 2002;25:275-8 ↩
The ADVANCE Collaborative Group. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. New Engl J Med 2008;358:2560-72 ↩
The ACCORD Study Group. Effects of intensive glucose lowering in type 2 diabetes. New Engl J Med 2008;358:2545-59 ↩
Lee Y, Lin Y, Leu W, et al. Sliding scale insulin used for blood glucose control: a meta-analysis of randomised controlled trials. Metabolism 2015;64:1183-1192 ↩
Vinik AI, Mitchell BD, Maser RL, et al. Diabetic autonomic neuropathy. Diabetes Care. 2003;26:1553-79 ↩
Ewing DJ, Clarke BF. Diagnosis and management of diabetic autonomic neuropathy. BMJ. 1982;285:916-918 ↩
Diem P, Laedarch-Hofmann K, Navarro X, et al. Diagnosis of diabetic autonomic neuropathy: a multivariate approach. Eur J Clin Investigation. 2003;33:693 ↩
Sahin M, Kayatas M, Urun Y, et al. Performing only one cardiovascular reflex test has a high positive predictive value for diagnosing autonomic neuropathy in patients with chronic renal failure on hemodialysis. Ren Fail. 2006;28:383-7 ↩
Schwab TM, Hendey GW, Soliz TC. Screening for ketonemia in patients with diabetes. Ann Emergency Med. 1999;34:342-6 ↩
Wallace TM, Matthews DR. Recent advances in the monitoring and management of diabetic ketoacidosis. Q J Med. 2004;97:773-80 ↩
Brandenburg MA, Dire DJ. Comparison of arterial and venous blood gas values in the initial emergency department evaluation of patients with diabetic ketoacidosis. Ann Emergency Med. 1098;31:459-65 ↩
Forsythe SM, Schmidt GA. Sodium bicarbonate for the treatment of lactic acidosis. Chest. 2000;117:260-7 ↩
Lutterman JA, Adriaansen AA van’t Laar A. Treatment of Severe Diabetic Ketoacidosis A Comparative Study of Two Methods Diabetologia.1979;17: 17-21 ↩
Hale PJ, Crase J, Nattrass M. Metabolic effects of bicarbonate in the treatment of diabetic ketoacidosis BMJ. 1984;289:1035-8 ↩
Morris LR, Murphy MB, Kitabchi AE Bicarbonate therapy in Severe Diabetic Ketoacidosis Ann Intern Med.1986;105:836-40 ↩
Gamba A, Oseguera J, et al. Bicarbonate therapy in severe diabetic ketoacidosis. a double blind, randomized, placebo controlled trial. Rev Invest Clin. 1991;43(3):234-238 ↩
Chua HR, Schneider A, Bellomo R. Bicarbonate in diabetic ketoacidosis – a systematic review. Annals Int Care 2011,1:23 http://www.annalsofintensivecare.com/content/1/1/23 ↩
Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA. 2005;293:217-28 ↩