
How Can We Help?
Venous thromboembolism and anticoagulation
Diagnosis of DVT and pulmonary embolus
Deep vein thrombosis. Venous thromboembolism (VTE) is common and treatable. Suspect it in any patient with sudden onset of calf pain and swelling, especially if there are predisposing factors such as prolonged immobility, active tuberculosis, pregnancy or malignancy. Measuring calf circumference is helpful if there is doubt about the swelling. Tender regional adenopathy suggests cellulitis, but pain along the femoral vein is common in extensive DVTs.
Pulmonary embolus Consider pulmonary embolus in a patient who presents with abrupt onset respiratory symptoms (cough, chest pain, shortness of breath), particularly if there are predisposing factors. (Remember to consider fat embolism in patients with dyspnoea and extensive bony fractures – petechiae on skin or subconjunctivae.)
The chest pain can be either pleuritic or angina-like. Haemoptysis is not common (about a third of patients) but very suggestive, particularly if the CXR looks normal. On examination there may be an obvious source such as a swollen calf, and varying degrees of respiratory compromise ranging from mild tachypnoea or wheeze to signs of consolidation and right heart failure. Presentation as acute pulmonary oedema is well described.1
The diagnosis is highly likely in a patient with abrupt onset dyspnea, no clinical features of LVF, and clear lungs on auscultation. The CXR may be normal or show non-specific infiltrates – the wedge shadow of pulmonary infarction is rare. The ECG shows a tachycardia and sometimes an RV strain pattern with ST changes in the early V leads. The so-called S1,Q3, T3 pattern is unusual, but a right axis shift is suggestive.

Treatment of DVT and pulmonary embolus
DVT – weight based heparin SC without PTT monitoring followed the next day by warfarin.
The subcutaneous heparin can either LMW or unfractionated. The latter is considerably cheaper but is becoming less readily available in strengths suitable for subcutaneous use. Heparin is conventionally given for at least five days, or until the INR is therapeutic if it is still not there yet by Day 5.
Pulmonary embolus – intravenous heparin infusion with 4 hourly PPT monitoring, initiate warfarin the next day
Perspective – CRP and DVT
Patients with DVT are often tested for measures of inflammation, and if these are elevated the question then arises whether an infection or malignancy (warranting careful investigation) is causing the elevated marker (usually the CRP) or if the DVT can cause this elevation on its own. The short answer is both, and a careful history and examination are always worthwhile. Inflammation is probably associated with DVT in observational studies2,3 but there is also time series information suggesting that the CRP rises with a DVT and settles shortly after, with values up to 50 mg/L on Day 2, usually settling to less than 20 mg/L by Day 54
Perspective – DVT and the use of D-Dimer testing.
If the pre-test probability is low and the D-dimer result is negative, NPV using ELISA tests is 99.4% (96.9-100%)5 A similar result was obtained in excluding pulmonary embolism with NPV of 99.5% (99.1-100%).6 The sensitivity falls to about 75% if the patient is already on warfarin (NPV 93%) and in all cases the positive predictive value is poor (about 45%) In addition, the older latex D-dimer tests can be used7in spite of their initial poor performance so long as an experienced technician performs the test immediately.
A pulmonary embolism clinical scoring system is as follows:8
- Score one point each for haemoptysis or the presence of malignancy
- Score 1.5 points each for a pulse above 100, a prior history of DVT/PE, or a story of immobilisation (e.g. surgery, bedrest > 3 days) in the last month.
- Score three points for clinical evidence of a DVT (swollen painful leg with pain on palpation over deep veins.)
- Add the points for any of these six features that are present. Then consider whether there is another more likely diagnosis. If there isn’t, add another three points.
If the total score is less than two, there is a low probability of PE; if it is greater than 6, the probability is high. Anything between two and six is ‘moderate’ probability. One point of this is that it facilitates making a treatable diagnosis on quite thin grounds – e.g. a tachycardia and history of recent surgery, with no more likely diagnosis would allow a PE label.
Perspective – prognostication in patients with pulmonary embolus.
Patients who are desaturating have a poorer prognosis. The probability of shock, respiratory failure or death in one study9 was 2% if saturation by pulse oximetry on room air were >95% and was 20% if saturation were less than 95%, giving a sensitivity of 90% and a specificity of 64% for this composite endpoint.
Perspective – chest wall pain on palpation in pulmonary embolism.
Finding an area of sharply localised pain over the chest wall in someone suspected of having a pulmonary embolus has traditionally been taken to mean that the diagnosis of PE is very unlikely, but a multi-centre study10 from France and Switzerland which enrolled 965 patients (222 had a PE) was reported as showing a sensitivity of 19% and a specificity of 79%, giving a LR+ of 0.83 and a LR- of 1.04. If this finding is reproduced in other studies, the sign should be discarded.
Perspective – ECG in pulmonary embolism
Although the ECG signs that are regularly mentioned do not perform terribly well diagnostically, there is some information on their prognostic value.11
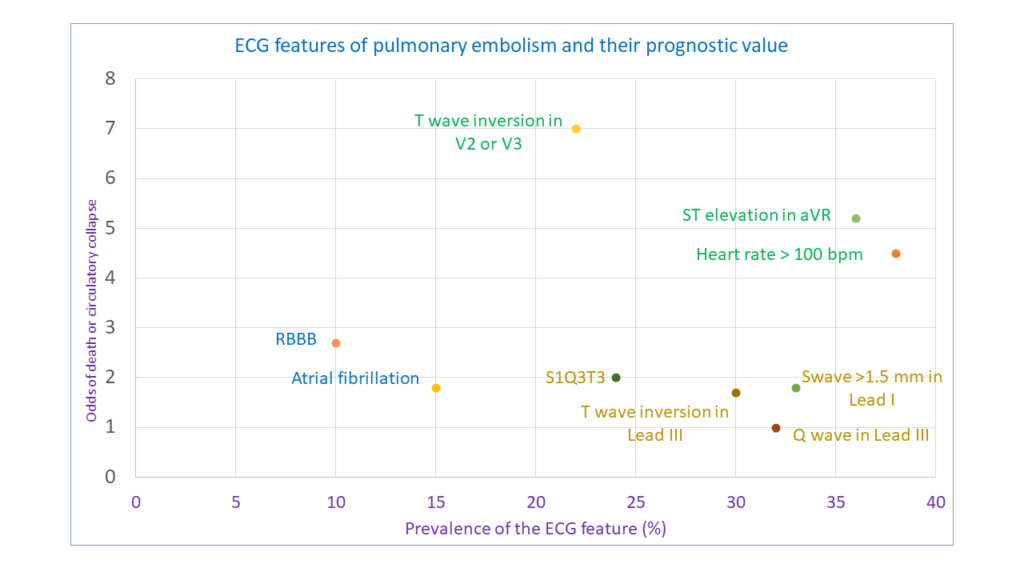
Thus, the typical S1Q3T3 pattern is far from typical, occurring in less than 25% of patients with a PE, but other findings of RV strain are also not that common, reflecting differences in size of the embolism (amount of pulmonary vasculature occluded). ST elevation in aVR is more common and if present, may suggest a bigger embolic load than S1Q3T3. However, diagnostically none of these signs are exclusive and can be found in other causes of acute RV strain such as asthma, cor pulmonale, severe chest infection and LV failure12.

S1Q3T3 pattern
Anticoagulation – indications
- Venous thromboembolic disease, including suspected or proven pulmonary embolism
- Potential left sided embolic disease – atrial fibrillation, mitral stenosis, severe cardiomyopathy, prosthetic heart valves.
- Hypercoagulable states – nephrotic syndrome, dehydration or immobility.
Anticoagulation in pulmonary embolism and DVT.
Severe pulmonary embolus with heamodynamic compromise.
Patients in whom the diagnosis of pulmonary embolism is very likely and who have features of haemodynamic compromise or hypoxaemia should be considered for streptokinase – use an initial bolus of 250 000 units in 200 ml saline over 30 minutes, followed by an infusion of 100 000 units per hour for the next 24 hours, followed by a conventional heparin infusion (don’t give the two simultaneously!)
Probable (or confirmed) pulmonary embolus but without haemodynamic compromise.
- LMW heparin – e.g enoxaparin 1 mg/kg 12 hourly (e.g. 80 mg 12 hourly for an 80 kg patient)
- IV unfractionated heparin infusion (not multiple IV bolus doses – this has the highest bleeding risk) with PTT monitoring, using an infusion pump or syringe driver. Start with a loading dose of 5000 units stat, then give 30 000 units at a rate to run over 24 hours, and adjust according to 4 hourly PTT to achieve a value 1.5 to 2.5 times greater than control – e.g. if control is 28 seconds, aim for patient result of 56s. One simple regimen would be 7500 units in 200ml saline to run over 6 hours. This is a bolus of 80 units per kg, followed by an infusion of 18 units per kg per hour.13
Deep vein thrombosis without obvious clinical PE.
Therapeutic options for DVT are:
- Weight-based subcutaneous low molecular weight heparin (LMW) without monitoring
- Weight-based subcutaneous unfractionated heparin without PTT monitoring
Perspective – what actually happens with unfractionated heparin?
The elegant attainment of perfect anticoagulation using intravenous heparin is somewhat difficult, a factor which is largely ignored by many guideline originators. A study from Harvard14 makes the point quite cogently: in 311 patients only 29% had three consecutive therapeutic PTTs, 54% had at least one prolonged interruption of the heparin infusion, and 4.8% had a major bleed.
This is a major reality check, and fits in with the experience of many clinicians attempting to give heparin infusions other than in an ICU.
Subcutaneous unfractionated heparin without PTT monitoring.
The use of unfractionated heparin subcutaneously without PTT monitoring is probably safe and effective, although this has only been demonstrated in a single randomised trial In resource constrained settings where LMW heparin is unavailable and where PTT monitoring cannot be done properly, it may be acceptable to default to an unmonitored regimen, although in patients with other comorbidities or haemodynamic instability this is untested and probably inadvisable. A sufficiently concentrated formulation is now rarely, and so this option (considerably cheaper than LMW heparin) is no feasible.
Low molecular weight heparin
The LMW heparins are dosed differently according to the particular agent: the dose of enoxaparin for the treatment of DVT is 1 mg/kg 12 hourly (e.g. 80 mg sc. 12 hourly for an 80 kg man), whereas dalteparin is 200 IU/kg once daily. At present these agents are still considerably more expensive than unfractionated heparin, and probably not much more effective. They are less likely to cause thrombocytopenia, but this is seldom a major clinical concern with short term use.
Perspective – efficacy of subcutaneous UF and LMW heparin in DVT and pulmonary embolus.
A group from Italy15 looked at the use of PTT-adjusted unfractionated heparin compared to a LMW heparin (nadroparin), both given subcutaneously. The trial was randomized but unblinded, and included a small number (14%) of patients with pulmonary embolism. Recurrent thromboembolism occurred in about 4% in each group, major bleeding in about 1% each and the overall mortality at 3 months was also similar (3.3%) With these lowish event rates the sample size was probably a bit small to confidently exclude a small real difference, but clearly neither option was dramatically more effective than the other.
Unfractionated subcutaneous heparin without PTT monitoring was compared to LMW heparin in a randomised open label but adjudicator-blinded Canadian study16 containing a large proportion of outpatients (70%). The initiating event was a DVT in 81% and a pulmonary embolus in 19%. There was equivalence between the two arms with remarkably similar outcome proportions to the Italian group. For unfractionated vs LMW heparin, recurrent thromboembolism rates were 3.8% vs 3.4%, and for major bleeding, 1.1% vs 1.4%. (Neither difference was statistically significant.) The unfractionated heparin loading dose was 333 units/kg followed by 250 units/kg 12 hourly. In 80% of patients on unfractionated heparin the PTT was therapeutic or supratherapeutic, but in this arm of the trial there were no episodes of major bleeding within 10 days of enrollment.
Another methodological twist in the LMW heparin tail is a report17 that of 15 trials of LMW heparin versus unfractionated heparin (IV) only 3 used a validated PTT range and 7/15 showed a reduction in heparin dose to < 30 000 IU per day in response to these PTT results, the implication being that the ‘control’ arm in many LMW trials may have been under-dosed.
Perspective – prophylactic anticoagulation in hospitalised medical patients
Heparin anticoagulation does reduce the rate of pulmonary embolism, but a meta-analysis of nine studies18 failed to demonstrate a statistically significant overall mortality advantage. The pooled group were at lowish risk (the control symptomatic DVT rate was 0.81%), but although the use of heparin halved this to 0.38%, this difference was not statistically significant. There was significant reduction in fatal pulmonary emboli (0.39% reduced to 0.14%, ARR 0.25%, NNT 400) and in the combination of fatal and no-fatal pulmonary emboli (NNT 345.)
The usual caveat applies: failure to demonstrate benefit is not the same as a demonstration of lack of benefit, because the absolute number of events in most trials was so low.
Prescribing warfarin.
Duration of warfarin therapy is dictated by aetiology, and is a balance between the risk of a recurrent event (highest in the first week, then tailing off rapidly for ‘once-off’ aetiologies) and the risk of bleeding (constant over time, but cumulative).
Probable aetiology | Desired INR | Duration of therapy |
A reversible cause like prolonged immobility and dehydration (e.g. a long taxi journey) | 2.0-3.0 | 6 weeks to 3 months |
Severe illness – e.g. cachexia and TB | 1.5-2.5 | 3 months |
Recurrent pulmonary emboli | 2.0-3.0 | Life long |
Warfarin dosing
Various guidelines have been published over the years to provide suggested warfarin doses.19 Consider:
- Body weight and patient age.
- Pharmacogenetics of warfarin metabolism – some individuals metabolise it faster than others.
- Drug interactions. In developing countries, it is important to consider these due to the high prevalence of tuberculosis and epilepsy. Rifampicin and phenytoin tend to lead to requirements for higher warfarin doses. (In the table below, the doses suggested in patients who have been taking rifampicin for more than 3 weeks are purely that – suggestions. The numbers shown are guesses and have not been formally validated but it is not rare to find individuals needing maintenance doses of 15 to 20 mg/day.)The dose on day 5 is usually the predicted maintenance dose.
The INR is only valid if the PTT is < 2.5 times control – it the patient is over-anticoagulated with heparin then the INR becomes unreliable.
Remember that using anticoagulants involves balancing two major risks – that of thromboembolism against the risk of a major bleed. For an INR > 2.0, the risk of a major bleed is about 14 per 1000 patient months. For a first episode of thrombosis, the thromboembolic risk at 3 weeks has already dropped to 20 per 1000 patient months, and by a month is less than 14.
The Fennerty protocol starts with 10 mg on the first day if the basal INR is less than 1.4. The INR is then checked again on the second day. If it is less than 2.0, a further 10 mg is given; if it is more than 2.0, warfarin is skipped for that day. On day three, the INR is again checked: if less than 2.0, give a further 10 mg; if 2.0 to 2.9, give 5 mg; if 3.0 to 3.4 give 2,5 mg, and if above 3.4, give none. On the fourth day, the dose adjustment is easier – give 7.5 mg if the INR is still less than 1.5; give 5 mg if it is between 1.5 and 2.5, and give 2.5 mg if it is above 2.5. If the patient is already on rifampicin, these doses may need to be increased, but there is little empiric support for the size of the increase.
Perspective: complications from anticoagulation with warfarin
It is conventionally accepted that the lower your INR, the less effective will be the anticoagulation in terms of events prevented, but the safer it will be in terms of bleeds prevented. This is extrapolated from the ‘other end’ of the therapeutic range, where, as the INR rises above 4, the risk of bleeding increases even though the risk of clotting events falls. A study from Canada20 casts some doubt on this. In this study, patients were divided into two groups, one with a target INR of 1.5 to 1.9, and the conventional dosing group where the target was 2.0 to 3.0. All patients had already been on warfarin for three months for ‘unprovoked’ DVT. While there was a statistically significant excess of recurrent venous thrombo-embolic events in the lower target INR group (19 per 1000 patient years versus 7) there was no difference in bleeding rates or mortality.
A meta-analysis21 gives another perspective on the frequency of complications of anticoagulation:
Complication | Rate per 100 person-years (95% CI) |
Any major bleeding | 7.2 |
Fatal bleeding | 1.3 |
Intracranial bleeding | 1.2 |
Intracranial bleeding occurring after 3/12 Rx | 0.7 |
Percentages | |
Intracranial bleeds as percent of all bleeds | 8.7% |
Mortality rate for major bleeds | 13.4% |
Mortality rate of intracranial bleeds | 45.8% |
This suggests that for every 100 patients adequately anticoagulated for a year, 7 will have a major bleed and one will die. Put even more succinctly, for every ten patients treated for a decade, one will die because of treatment during that time. It is important to ensure that the benefits of therapy clearly outweigh the risks for each individual patient!
Perspective – how good are dosing regimens?
A systematic review22 found little to choose between 10 mg and 5 mg loading doses, although 5 mg seemed to work as well if the INR was checked frequently. The Fennerty protocol was unimpressive in the elderly compared to age-adjusted dosing (proportion achieving a stable INR 22% versus 48%.)
Perspective – skin necrosis and starting warfarin without starting heparin first.
Besides the well-known vitamin K dependent clotting factors, the liver also manufactures anti-coagulants such as protein C and protein S and antithrombin III. In persons with either congenital or acquired deficiencies of these, adding warfarin without heparin first can result in a transient hypercoagulable state, as the different factors have different half-lives, so it is possible to reduce production of anticoagulants while pro-coagulants are still lingering on.
This can result in spontaneous coagulation which usually rather strikingly happens in the skin, for unclear reasons. Various size areas of skin infarct, giving the equivalent of a third degree burn in that area. The management is to stop the warfarin, give heparin, and then possibly cautiously re-introduce the warfarin (e.g. starting with 2.5 mg alt days) once the patient is very thoroughly anticoagulated with heparin.23
Perspective – duration of anticoagulation
An often quoted study24 suggests benefit from ongoing low dose anticoagulation in patients already given six months of warfarin. In this study the INR was kept at 1.5-2.0 for an average of a further 2 years, and showed a reduction in risk from 7.2 thromboembolic events per 100 person-years on placebo to 2.6 on warfarin. The characteristics of the patients in this study are worth remembering, however. The median age was 53, but median BMI was 29.9, and nearly 40% had had 2 or more previous VTEs. About 25% were positive for Factor V Leiden. Another cohort from Italy25 (1626 patients followed for up to 10 years) found a recurrence rate of 52% in those with unprovoked (spontaneous’) DVTs versus 22% for provoked (there was a cause found.)
A subsequent meta-analysis26 found fewer recurrences in patients treated for longer courses (usually 6 months or more) versus shorter courses (usually 1-3 months) but the incremental risk reduction from continuing beyond 6 months was quite modest. It was suggested that the NNT for longer rather than shorter anticoagulation in order to prevent one VTE was 50, with a wide confidence interval (25-1000). Another study27 of 619 patients found that patients with an elevated D-dimer level 30 days after stopping warfarin had a hazard ratio of 4.26 (1.23 – 14.6) for VTE recurrence, and there was some evidence to support resuming anticoagulation in such patients.
It is important to consider the bleeding risk to – hospitalisation for bleeding happens in about 10% of patients in the first six months on warfarin, and then at a rate of 3% per year thereafter.
General recommendations for warfarin duration are about 3-6 months for a provoked DVT and longer, even life-long, depending on the patient’s individual risk profile, if idiopathic.
Anticoagulation and surgery
Patients already on warfarin
Individuals with fresh (less than one month) venous or arterial thrombosis should have warfarin stopped till the INR has dropped to ‘safe’ levels (e.g. 1.3 or less – surgeon’s decision) and be covered during that period with formal intravenous heparin anticoagulation before surgery and then after surgery until the warfarin is therapeutic again. Most other patients who are on warfarin can have the warfarin stopped for a few days before surgery and then post-operatively can be put on subcutaneous heparin while waiting for the recommenced warfarin to start to work.
Prophylactic anticoagulation
Higher risk patients not already on an anticoagulation regimen should be considered for prophylactic subcutaneous unfractionated heparin – e.g. 5000 units 2 or 3x/d. This does not require PTT monitoring.
Perspective – anticoagulation and surgery.
There is often considerable uncertainty about the management of patients who have been on warfarin and who now require surgery. Surgery is probably safe with an INR of 1.528 but it takes three to four days after discontinuing warfarin for a therapeutically anticoagulated patient to reach this level. It will take about another three days for the INR to reach 2 on re-starting treatment. Some indication of the risks involved:29
- DVT. Without treatment, the recurrence risk is 40% in the first month, and then drops to 10% in the second and third months. Patients may be continued on anticoagulation beyond three months if at high risk, and in this case the risk is estimated at 15% per year. Relative risk reduction with warfarin: 80%. Hence ARR for the first month is 32% and NNT is 4, ARR for months 2 and 3 is 8% and ARR is 13.
- In non-valvular atrial fibrillation, the risk is 4.5% per year unless there has been a previous episode of embolisation, in which case the risk is 12% per year. Relative risk reduction with warfarin: 66%. Hence ARR about 3% and NNT 34 per year.
- Patients with a mechanical heart valve not on warfarin have a risk of about 8% per year, but this is dependent on the type of valve. Relative risk reduction with warfarin: 75%. ARR 6%, NNT 17 per year.
- In the first month after an arterial embolism, the risk of recurrence is 15%. Relative risk reduction with warfarin: 66%. ARR 10%, nnt 10.
If intravenous heparin is indicated, stop it 6 hours before surgery and re-start it 12 hours after surgery. A possible management strategy is: (modified from Kearon and Hirsch)
- For acute DVT less than a month previously, stop warfarin and give IV heparin before (stop 6 hours pre-operatively) and after surgery (start 12 hours post-operatively.)
- For DVT 2 to 3 months previously, stop warfarin before surgery and give IV heparin post-operatively only (commence 12 hours after surgery, and without a loading dose.)
- For atrial fibrillation or prosthetic heart valve, stop warfarin pre-operatively and give subcutaneous heparin post-operatively in prophylaxis doses.
In all cases where ongoing warfarin therapy is indicated, re-start it as soon as the patient is able to take orally.
Some further empiric support for this recommendation comes from an observational cohort30 of 1024 patients with 1293 episodes of warfarin interruption for outpatient surgical procedures. Only 8.3% were given bridging heparin. The incidence of thromboembolism within 30 days of the procedure was 0.5% for those not given heparin, and nil in those given heparin. However the incidence of clinically important bleeding in those given heparin was 13%.
Screening for thrombophilias.
There are some features that make it more likely that a secondary cause (protein C, protein S, anti-thrombin C, etc) will be found, and these include age less than 50 years, recurrent thrombosis, and a family history of thrombosis. In the absence of these and in the presence of another strong short-term risk factor (e.g. surgery, tuberculosis) it is probably not necessary to screen for thrombophilias. The other strong argument against screening is the need to decide on level and duration of anticoagulation on clinical features anyway. If you have already decided that a patient needs warfarin for life on the basis of recurrent pulmonary thromboembolism, then demonstrating heterozygosity for factor V Leiden will do little to change management.
A reasonable screen for antiphospholipid antibody syndrome is to do an INR, PTT and anticardiolipin Ab test. If all these are negative then it is unlikely that the patient has APS.
Perspective – risk of venous thrombosis with various clotting factor abnormalities:
Against a normal population risk of 0.008% thrombosis per year, the risk in those with hyperhomocysteinaemia is 0.02% per year, the oral contraceptive risk is 0.03%, the factor V Leiden heterozygote risk (very rare in Africa and Asia, but up to 10% prevalence in those of North European descent with DVTs ) is 0.06%. Protein C, Protein S, V Leiden homozygote and antithrombin C deficiency are all an order of magnitude more likely to develop thrombosis, with rates of 0.5 to 1% per year. However, their prevalence in patients with first episodes of DVT is usually reported as less than 5%.
By screening for all three of proteins C and S and antithrombin deficiency in DVT patients there is a 4-20% chance of picking up one of these diseases that you are going to manage on clinical grounds with warfarin in any case. If you do have a patient with one of these deficiencies which you don’t know about, whom you are seeing with a first episode, then stopping warfarin after the conventional period is still reasonable as a recurrence is more likely to be a DVT than a pulmonary embolus.
Jobe RL, Forman MB. Focal pulmonary embolism presenting as diffuse pulmonary edema. Chest. 1993;103(2):644-646. doi:10.1378/chest.103.2.644 ↩
Grimnes G, Isaksen T, Tichelaar YIGV, Brox J, Brækkan SK, Hansen JB. C-reactive protein and risk of venous thromboembolism: results from a population-based case-crossover study. Haematologica. 2018 Jul;103(7):1245-1250. doi: 10.3324/haematol.2017.186957. Epub 2018 Apr 19. PMID: 29674505; PMCID: PMC6029539 ↩
Fox EA, Kahn SR. The relationship between inflammation and venous thrombosis. A systematic review of clinical studies. Thromb Haemost. 2005 Aug;94(2):362-5. doi: 10.1160/TH05-04-0266. PMID: 16113826. ↩
Roumen-Klappe EM, den Heijer M, van Uum SH, van der Ven-Jongekrijg J, van der Graaf F, Wollersheim H. Inflammatory response in the acute phase of deep vein thrombosis. J Vasc Surg. 2002 Apr;35(4):701-6. doi: 10.1067/mva.2002.121746. PMID: 11932666. ↩
Kearon C, Ginsberg JS, Doukets J, et al. Management of suspected deep vein thrombosis in outpatients by using clinical assessment and D-dimer testing. Ann Intern Med 2001;135:108-111 ↩
Wells PS, Anderson DR, Rodger M, et al. Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and D-dimer. Ann Intern Med. 2001;135:98-107 ↩
Schutgens RE, Usseboom EU, Haas FJ, et al. Usefulness of a semiquantitative D-dimer test for the exclusion of deep vein thrombosis in outpatients. Am J Med. 2002;112:617-621 ↩
Wells PS, Ginsberg JS, Anderson DR, et al. Use of a clinical model for safe management of patients with suspected pulmonary embolism. Ann Intern Med. 1998;129:997-1005. ↩
Kline JA, Hernandez-Nino J, Newgard CD, et al. Use of pulse oximetry to predict in-hospital complications in normotensive patients with pulmonary embolism. Am J Med. 2003;115:203-8 ↩
Le Gal G, Testuz A, Righini M, et al. Reproduction of chest pain by palpation: diagnostic accuracy in suspected pulmonary embolism. BMJ. 2005;330:452-3 ↩
Shopp, J., Stewart, L., Emmett, T., & Kline, J. (2015). Findings From 12-lead Electrocardiography That Predict Circulatory Shock From Pulmonary Embolism: Systematic Review and Meta-analysis. Acad Emerg Med, 22(10), 1127-1137. http://dx.doi.org/10.1111/acem.12769 ↩
Marchick MR, Courtney DM, Kabrhel C, Nordenholz KE, Plewa MC, Richman PB, Smithline HA, Kline JA. 12-lead ECG findings of pulmonary hypertension occur more frequently in emergency department patients with pulmonary embolism than in patients without pulmonary embolism. Ann Emerg Med. 2010 Apr;55(4):331-5. doi: 10.1016/j.annemergmed.2009.07.025. Epub 2009 Sep 19. PMID: 19766353. ↩
Raschke RA, Reilly BM, Guidry JR, et al. The weight-based heparin dosing nomogram compared with a “standard care” nomogram. Ann Intern Med. 1993;119:874-81 ↩
Hylek EM, Regan S, Henault LE, et al. Challenges to the effective use of unfractionated heparin in the hospitalised management of acute thrombosis. Arch Intern Med 2003;163:621-7 ↩
Writing Committee for the Galilei Investigators. Subcutaneous adjusted-dose unfractionated heparin vs. fixed dose low-molecular-weight heparin in the initial treatment of venous thromboembolism. Arch Intern Med 2004;164:1077-83 ↩
Kearon C, Ginsberg JS, Julian JA, et al. Comparison of fixed-dose weight-adjusted unfractionated heparin and low-molecular-weight heparin for acute treatment of venous thromboembolism. JAMA. 2006;296:935-42 ↩
Raschke R, Hirsh J, Guidry JR. Suboptimal monitoring and dosing of unfractionated heparin in comparative studies with low-molecular weight heparin. Ann Intern Med. 2003;138:720-3 ↩
Dentali F, Douketis JD, Gianni M, et al. Meta-analysis: anticoagulant prophylaxis to prevent venous thromboembolism in hospitalised medical patients. Ann Intern Med. 2007;146:278-88 ↩
Fennerty A, Campbell IA, Routledge PA. Anticoagulants in venous thromboembolism. BMJ 1988;297:1285-87 ↩
Kearon C, Ginsberg JS, Kovacs MJ, et al. comparison of low-intensity warfarin therapy with conventional-intensity warfarin therapy for long-term prevention of recurrent venous thrombo-embolism. N Engl J Med.2003;349:631-9 ↩
Linkins L, Choi PT, Douketis JD. Clinical impact of bleeding in patients taking oral anticoagulant therapy for venous thromboembolism. Ann Intern Med. 2003;139:893-900 ↩
Heneghan C, Tyndel S, Bankhead C, et al. Optimal loading dose for the initiation of warfarin: a systematic review. BMC Cardiovascular Disorders. 2010;10:18 ↩
Stewart AJ, Penman ID, Cook MK, et al. Warfarin-induced skin necrosis. Postgrad Med J. 1999;75:233-5 ↩
Ridker PM, Goldhaber SZ, Danielson E, et al. Long-term low-intensity warfarin therapy for the prevention of recurrent venous thromboembolism. N Engl J Med. 2003;348:1425-34 ↩
Prandoni P, Noventa F, Ghirarduzzi A, The risk of recurrent venous thromboembolism after discontinuing anticoagulation in patients with acute proximaldeep vein thrombosis or pulmonary embolism: a prospective cohort study in 1,626 patients. Haematologica. 2007;92:199 –205 ↩
Ost D, Tepper J, Mihara H, et al. Duration of anticoagulation following venous thromboembolism. JAMA. 2005;294:706-15 ↩
Palareti G, Cosmi B, Legnani C, et al. D-dimer testing to determine the duration of anticoagulation therapy.N Engl J Med. 2006;355:1780-9 ↩
White RH, McKittrick T, Hutchinson R et al. Temporary discontinuation of warfarin therapy: changes in the international normalised ratio. Ann Intern Med. 1995;122:40-42 ↩
Kearon C, Hirsh J. Management of anticoagulation before and after elective surgery. N Engl J Med. 1997;336:1506-10 ↩
Garcia DA, Regan S, Henault LE, et al. Risk of thromboembolism with short-term interruption of warfarin therapy. Arch Intern Med. 2008;168:63-9 ↩
Bauer KA. The thrombophilias: well-defined risk factors with uncertain therapeutic implications. Ann Intern Med. 2001;135:367-73 ↩